


Measuring the Mandates: Lockdowns
Measuring the Mandates: Lockdowns

This article is the first chapter of Measuring the Mandates: Questioning the State’s Response to COVID-19. The full book is available here.
‘Deaths Soar In Country That Didn’t Lock Down.’
CNN Headline, 29th April, 2020
The dawning of a new decade may bring with it a sense of optimism. For our current one, there was something exciting about living in the twenties, with its historic connotations of social liberation and celebration. If at a New Year’s Eve party, someone had prophesied that the majority of the world’s liberal democracies would soon be imposing business closures and a form of house arrest on their citizens, they would have appeared quite mad.
The ‘roaring’ 1920s took over nine years to crash. Ours did so within three months.
The consequences of lockdowns were as brutal as they were predictable. The United Nations warned of ‘multiple famines of biblical proportions’, that would kill ‘hundreds of thousands of children’ whilst Oxfam cautioned that ‘the economic crisis is potentially going to be even more severe than the health crisis’, moving half a billion people into poverty. The inevitable rise in child trafficking was not long in coming. Commenting on cutbacks in essential medical care; the BBC speculated that ‘most COVID-19 deaths won’t be from the virus’ The Daily Mail reported that hundreds of cancers were being missed each week because screening had been suspended.
The implications of isolation for the elderly scarcely need pointing out, yet it is worth doing so anyway. To quote from Amnesty International’s report on the UK Government's abuse of the elderly once more:
‘After not seeing mum for months I found her terribly weakened, both physically and mentally. We were sitting in the garden several metres apart and she was crying all the time. Communicating at a distance is exhausting for her as she can’t hear properly. Mum doesn’t have dementia and before Covid used to have a lot of visitors, friends who live nearby visited every day. Now she has lost the will to live.’
And:
‘For five and a half months I only had window visits and during the last window visit I touched my mum’s hand through the small window opening, having first used hand sanitizer. I did so because mum was in pain and was crying. A carer saw this and my mum was put in isolation for two weeks. My mum already had COVID two months earlier and both my mum and I tested negative two days after the incident, but despite this she was still kept in isolation for the full two weeks. This is unnecessary and cruel. Before lockdown my mum was mobile and I used to take her out often, but since lockdown she has been kept in a wheelchair and has deteriorated sharply. Yesterday I had the first garden visit and for the first time she could no longer have a conversation.’
What could justify the implementation of a policy guaranteed to cause millions of deaths, decimate the global economy and deprive people of all quality in their lives? Surely the precautionary principle would demand overwhelming evidence that the policy would save substantially more lives than it destroyed? What was the historical precedent for this?
Even if the pessimistic New Year’s reveller mentioned above had been a student of pandemic preparedness, it’s unlikely he would have been able to predict lockdowns. World Health Organization public health measure advice as of 2019 recommends the voluntary isolation of sick individuals in their homes. Even in doing so, it acknowledges this poses an increased risk of infection to those cohabiting, and that ‘older adults who live alone may not receive sufficient care and support when home isolation is implemented’. The report further acknowledges that the effectiveness of isolation is ‘moderate’, and that the quality of evidence supporting it is ‘very low’. The duration of isolation is reckoned to be between five and seven days.
The quarantining of exposed individuals is not recommended, due to ethical considerations, a very low quality of evidence and ‘no obvious rationale for this measure.’ The mandatory quarantining of an entire population of healthy individuals is not even considered.
School and workplace closures and avoiding crowds are all ‘conditionally recommended’ in extreme circumstances. This semi-recommendation comes with the caveat that these interventions obviously bring their own harms, and that there is ‘very low’ overall quality of evidence that they reduce transmission.
International travel restrictions are conditionally recommended ‘during the early stage of a localised extraordinarily severe pandemic for a limited period of time’, with the same caveats as above. Full border closures are not recommended, due to ‘very low quality of evidence, economic consequences, resource implications and ethical implications.’
These were the positions of the WHO when the Chinese Communist Party (CCP) alerted them to an outbreak of viral pneumonia on the 31st of December, 2019.
On the 23rd of January, the CCP ordered a lockdown of fifty eight million people in Hubei province. At this point a total of eighteen people had been classified as dying of COVID-19 in Wuhan. Wuhan has a population of around nine million and is known as Smog City. The CCP had violently suppressed protests there over air pollution, which does not seem to have been considered a factor in these deaths.
At this time, strange videos emerged of people purportedly from Wuhan dropping dead in the streets. Whether these were deliberate propaganda or just the internet doing its thing is unknown, but they had the effect of terrifying the world.
At this time, there was still no indication that Western health authorities favoured lockdowns, with Anthony Fauci commenting on the 28th of February:
‘That’s something that I don’t think we could possibly do in the United States, I can’t imagine shutting down New York or Los Angeles, but the judgement on the part of the Chinese health authorities is that given the fact that it’s spreading throughout the provinces... it’s their judgement that this is something that in fact is going to help in containing it. Whether or not it does or does not is really open to question because historically when you shut things down it doesn’t have a major effect.’
The WHO acknowledged the uniqueness of the CCP approach, saying:
‘It has not been tried before as a public health measure, so we cannot at this stage say it will or will not work….The lockdown of 11 million people is unprecedented in public health history, so it is certainly not a recommendation the WHO has made.’
On the 30th of January Italy’s Prime Minister, Giuseppe Conte, declared a six month state of emergency after two Chinese tourists from Wuhan fell ill and tested positive for COVID-19. Conte was president of Italy’s Five Star Movement (M5S), which for the previous two years had sought closer economic ties to China.
Perhaps strangely, these closer ties involved healthcare. A Plan of Action on Health Cooperation between the two countries had been signed in March of 2019, and further updated in November. This included cooperation in the ‘prevention of infectious diseases.’ This was a continuation of health cooperation plans between Italy and China first launched in the year 2000, by former Prime Minister Massimo D’Alema, a one time member of Italy’s Communist Party. It is worth mentioning that D’Alema now serves as honorary president of the Silk Road Cities Alliance, a Chinese state organisation.
On the 22nd of February, fifteen cases of COVID were detected, and a fifteen day lockdown was implemented in the northern provinces of Lombardy and Veneto to ‘slow the spread.’ This was on the basis of the deaths of seven people, the overwhelming majority of whom were elderly people who had also been suffering from other health issues. To put that in context; an average February in Italy sees somewhere between fifty and sixty thousand deaths. The entire country would follow the north into lockdown on March the 9th.
Italy had leapfrogged China to put nearly sixty million people in lockdown, the largest lockdown in human history. It is only after the lockdowns were in effect that the excess mortality appeared.

The red dots in the graph are each February, the yellow line is set at the level of February 2022. No excess mortality is detectable.
As explored in Chapter One, excess deaths in Italy were severely imbalanced towards the north of the country and likely substantially iatrogenic in nature.
Central to Italy’s lockdown policy was Health Minister Roberto Speranza. Speranza was labelled ‘the most left-wing health minister in Italian history’. In October 2020, he published a book, Because we will Heal: From the Hardest Days to a New Idea of Health. The book was written during the summer, when excess mortality in Italy had receded. It was hastily withdrawn from sale due to the death rate spiking again that same month. Ostensibly this was because Speranza was too busy to devote time to presentations, but it has never gone back on sale, indicating the premature celebration of success had become embarrassing.
Attorney Michael Senger, author of Snake Oil: How Xi Jinping Shut Down the World, proposes that Speranza might have scrapped his book due to it being too candid about his ideological reasons for locking sixty million people down. Speaking of the Lombardy and Veneto lockdown, Speranza writes:
‘This is a measure with worrying implications for the economic and social fabric, but also with a terrible symbolic impact. Restricting citizens’ freedom of movement, sending the army to check that closures are respected. Could the protection of the right to health, recognized by Article 32 of the Constitution, lead us to restrict other fundamental rights guaranteed by the Constitution? And then, will this type of intervention really work, to stop the contagion? No other Western country has yet experienced this virus and the management strategies it requires. The only precedent we can look to is China, with a very different cultural, political and institutional model from ours. In Italy, everyone has been saying for weeks, it would be impossible to do what China has done. But what if it were necessary?’
In spite of Speranza describing himself as ‘a staunch rationalist’ who has a ‘true faith in science’, it is clear that no science underpinned Italy’s lockdown, only the recommendation of the Chinese Communist Party. One study was commissioned, using Chinese data, but was never published.
Speranza’s book reveals his ideological drives:
‘I am convinced that we have a unique opportunity to entrench a new idea of the left, based on a commitment that today everyone recognizes is needed: to defend and relaunch fundamental public goods’
‘We have experienced unbridled individualism, we have undergone its economic and social translation: neoliberalism as well so unbridled.‘
‘Individualism has weakened social networks and fragmented representation. It was thought that the state was no longer needed, that it should be reduced to a minimum.That all his interference was a nuisance because society and the economy were able to regulate themselves. They just had to be left “free.”’
‘The months of Covid, however, have accelerated a rethinking process of which some first signs were already visible. We have rediscovered how important fundamental public goods are, starting with the protection of health. For the first time, after many years, the left is not going against the wind. We have been in the long phase in which history seemed to go in the direction of neoliberal individualism, and in our going against the wind, looking for the route, fighting against solutions that were a bit messy and that had little to do with values of the left, in Italy we have experienced a painful split in the main center-left party. Today things are changing and an idea of the left can be reaffirmed starting from fundamental public goods and a new role of the state.’
As China made unthinkable lockdowns possible in Italy, so Italy opened the possibility for the rest of the world.
Suddenly the World Health Organization changed its tune. Abandoning it’s pandemic preparedness advice of only five months earlier declared:
‘The measures China has taken are good not only for that country but also for the rest of the world.’
This was at a time when China was reporting one hundred and seventy deaths from COVID-19 (not enough to make a dent in typical pneumonia deaths from Hubei province) and welding people inside their homes, causing some to be burnt alive.
WHO director-general Dr. Tedros Adhanom Ghebreyesus, a man who had once been a member of the most oppressive governments in the world, now said:
‘In many ways, China is actually setting a new standard for outbreak response. Our greatest concern is the potential for the virus to spread to countries with weaker health systems, and which are ill-prepared to deal with it.’
On the 24th of February, the World Health Organization declared:
‘China didn’t approach this new virus with an old strategy for one disease or another disease. It developed its own approach to a new disease and extraordinarily has turned around this disease with strategies most of the world didn’t think would work . . . What China has demonstrated is, you have to do this. If you do it, you can save lives and prevent thousands of cases of what is a very difficult disease.’
Scientists who had been pro-lockdown for years now seized the opportunity. Neil Ferguson led a study on case rates in the lockdowned town of Vo’, Italy. Professor Ferguson claimed to show that it had been effective, which influenced the decision to lockdown all of Italy on March the 9th. The study was based on testing for infections, which were demonstrably in decline before the lockdown had started. To quote Michael Senger:
‘Ferguson justified the lockdown of the United Kingdom based on the lockdown of Italy, which had in turn been justified with a false study led in part by Ferguson himself.’
Much like Roberto Speranza with China, Professor Ferguson credited Italy with making lockdowns possible:
‘It’s a communist one party state, we said. We couldn’t get away with it in Europe, we thought… and then Italy did it. And we realised we could.’
White House Coronavirus Response Coordinator Dr. Deborah Birx wrote of how she became convinced of the need to lockdown after seeing videos from China—videos that were soon conclusively proven to be propaganda:
‘We had to make these palatable to the administration by avoiding the obvious appearance of a full Italian lockdown. At the same time, we needed the measures to be effective at slowing the spread, which meant matching as closely as possible what Italy had done—a tall order.’
The initial justification for lockdowns was not to stop the virus passing through society, but to slow the spread so that hospitals would not be overwhelmed. Birx also admits that the ‘fifteen days to stop the spread’ was a lie:
‘No sooner had we convinced the Trump administration to implement our version of a two-week shutdown than I was trying to figure out how to extend it. Fifteen Days to Slow the Spread was a start, but I knew it would be just that. I didn’t have the numbers in front of me yet to make the case for extending it longer, but I had two weeks to get them. However hard it had been to get the fifteen-day shutdown approved, getting another one would be more difficult by many orders of magnitude.’
By April, more than half the world’s population—some 3.9 billion people—had been placed into lockdown.
It is clear that this policy, created and promoted by one of the world’s most authoritarian regimes, had no real scientific underpinning and was pushed for ideological reasons by people who were entirely aware of the devastating consequences. Even if there hadn't been a deadly virus circling the world, lockdown policies—taken in totality—were guaranteed to kill millions of people. Some of those deaths would be realised immediately, such as the ones arising from denial of healthcare, others would take weeks, such as starvation in the Third World, whilst still more would manifest over years to come, such as cancer deaths and the loss of services due to economic contraction. To say it again: all of this was entirely apparent at the time.
To quote Michael Senger once more:
‘The world has been fighting a virus from China with a public health policy from China that transforms the world into China.’
How could this be justified? Only through the claim that lockdowns would save more lives than they cost. Absent evidence, this is simply a gamble, so was it a gamble that paid off?
Lockdown efficacy
There are no shortage of claims that lockdowns saved millions of lives. If a strong form of the iatrogenic hypothesis explored in Chapter One is correct, whereby deaths attributed to COVID-19 were overwhelmingly caused by changes to medical systems, then lockdowns obviously did not save a single life. Their power could only have been destructive.
A case for this can certainly be made from the data. Various scientific studies have found evidence that the COVID-19 virus was present around the world for months before its sudden emergence as a killer. In Italy, it has been identified as far back as September 2019. This seems hard to reconcile with the fact that none of the countries supposedly strongly affected by COVID, saw any increased mortality prior to March 2020. More specifically, they did not see any prior to the implementation of lockdowns.
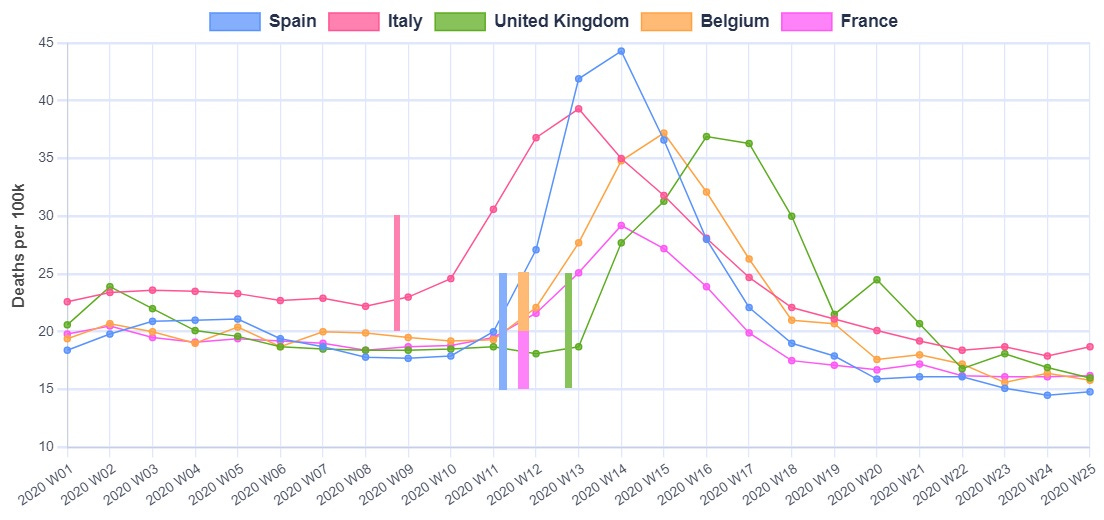
The graph below shows five European countries that experienced high excess mortality beginning in March 2020. The vertical bars indicate the various dates these countries imposed stay-at-home orders. This is an imperfect starting point, as it is not the act of staying home that causes excess deaths, but as the most extreme measure, stay-at-home orders are likely to have come shortly after changes to medical systems.
It is clear that lockdowns always precede excess mortality. Italy went into lockdown earlier than the other countries, and its excess deaths came proportionately earlier too. At the other end of the scale, the United Kingdom instituted lockdowns last, and was the last to see a mortality spike.
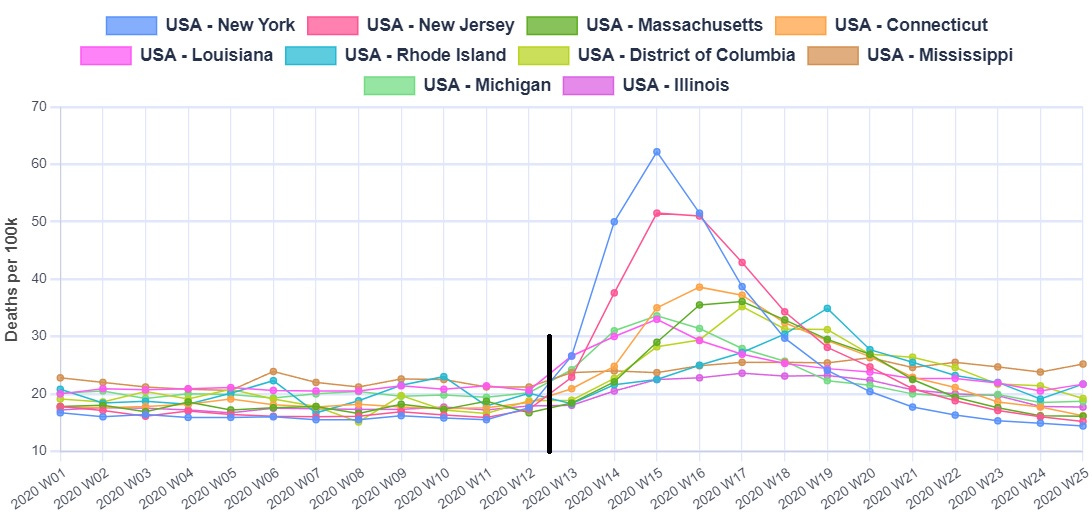
The picture is similar in the United States. The graph below shows the ten States which initially had the highest excess mortality. The black line is the date States issued stay at home orders or recommendations (plus or minus a couple of days). The same pattern as seen in Europe emerges, where no excess deaths are visible prior to lockdown, but a sudden spike comes immediately after. Europe's death spikes come just a few days prior, with the UK being slightly later.
By June of 2020, Dr. Anthony Fauci had been thoroughly won over to the lockdown cause, saying:
‘If you look at the data, now that papers have come out literally two days ago, the fact that we shut down when we did and the rest of the world did, has saved hundreds of millions of infections and millions of lives.’
Dr. Fauci is most likely referring to a collection of papers published just a few months after lockdowns were mandated, that claimed to demonstrate this saving of ‘millions of lives’. The papers were based on modelling speculative predictions of how COVID might travel and how lethal it might be. They did not take into account iatrogenic deaths or the more long term deaths that would be caused by lockdowns. They also do not seem to comport well to observations of the real world.
If lockdowns really had saved millions of lives in such a short period, then the effect would be impossible to miss. Indeed the world’s media predicted as much at the time. Any country eschewing this policy would suffer cataclysmic consequences, unmissable in both the data and anecdotal observations.
Is such a cataclysm visible?
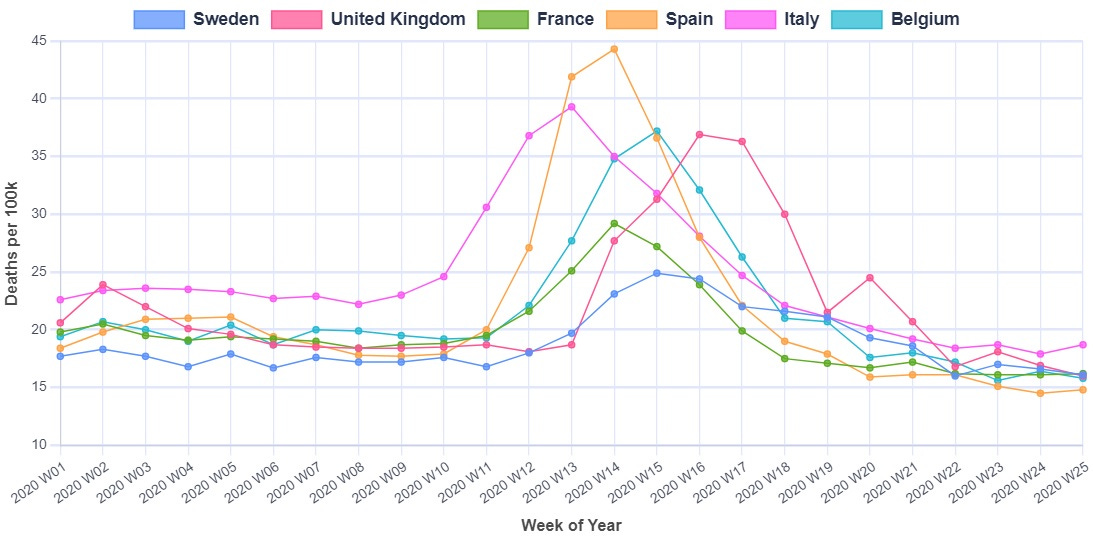
The ‘Deaths Soar In Country That Didn’t Lock Down’ quotation that opens this chapter is a CNN headline referring to Sweden. It is true that Sweden did not lockdown and deaths did indeed soar, but does the relationship that CNN implies actually exist?
If Sweden is added to the previous graph of the five European countries that did lockdown, it is clear that the initial period of excess mortality rose and fell away again at about the same rate. This means that, in spite of understandable public perception to the contrary, lockdowns cannot be credited with bringing the death rate under control.
Over half of the Swedish deaths at this time occurred in nursing homes, and it is clear iatrogenic factors played a substantial role. The country experienced no excess mortality in the under seventy fives during 2020, so whilst there are doubtlessly many thing Sweden could have done (or better to say, not done) to reduce their excess mortality, it is unclear how locking down younger people could have contributed.
Supporters of lockdowns have claimed that Sweden should be compared to its Nordic neighbours, rather than Europe in general. When this comparison is made, it is clear Sweden did comparatively badly during 2020, with two big spikes in excess mortality.
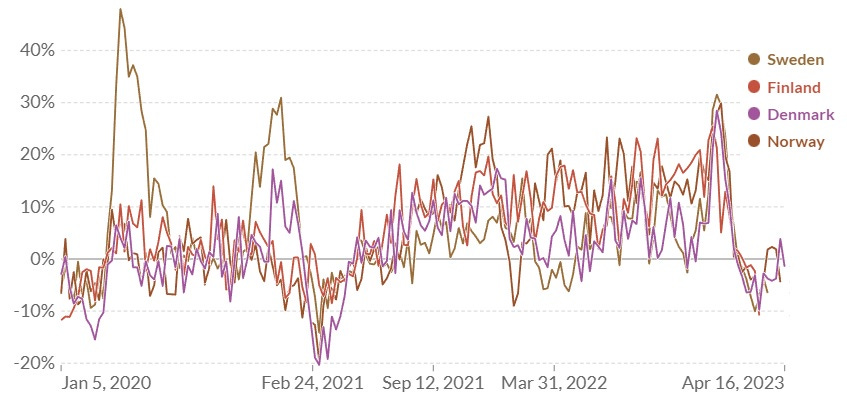
From February of 2021 onwards however Sweden’s excess was consistently lower than its neighbours. By June of 2022, the UK Office of National Statistics reported that Sweden was tied with Norway for lowest excess deaths in Europe since the beginning of the pandemic period.
Of course many countries instituted stay-at-home orders and did not instantly see an increase in excess mortality. It is claimed this is because they locked down before the virus had time to spread, and other countries would have had the same results if only they’d locked down sooner. To justify this claim however, it would have to be known what medical policies these countries had in place. An absence of excess mortality would indicate that, at least at this stage, they were not denying medical care to their elderly the way the, for example, United Kingdom was.
The United States provides an interesting—yet challenging—basis for comparison. Different States locked down in different ways for different periods of time. The bar chart below contains the deaths attributed to COVID-19 as of August 19th 2020, essentially the point where most States had concluded their first phase of lockdowns. The red dots are the states considered to have not locked down, or at least where restrictions were mildest:

It can of course be argued that not enough time had elapsed to gain a clear picture, this graph is clearly not what the lockdown supporters were claiming would happen in March 2020.
After two years had elapsed, a working paper published in the National Bureau Of Economic Research found that excess mortality was: ‘greater in US states where obesity, diabetes, and old age were more prevalent before the pandemic’, and that; Economic activity was less in states that had been intensive in, especially, accommodations and food. When these factors were controlled for, they found no relationship between reduced economic activity (a proxy for lockdowns) and excess mortality:
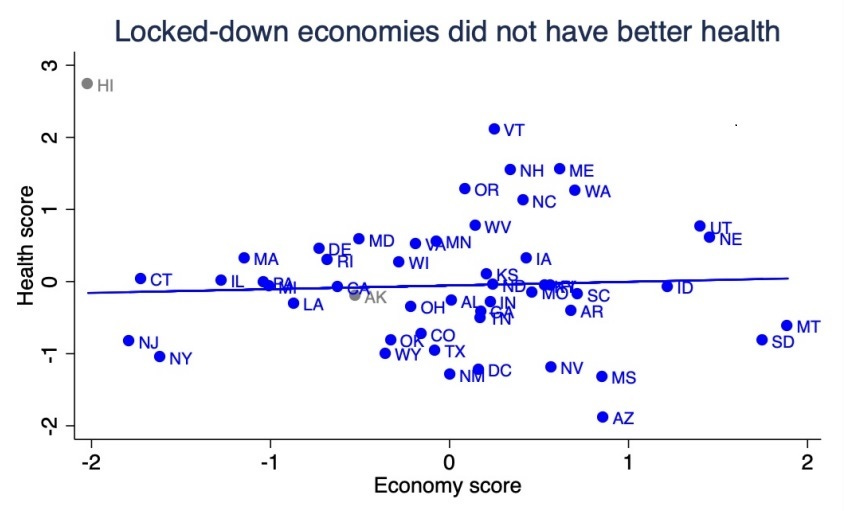
Whilst there are obviously a million ways to cherry-pick data, once pre-existing health conditions are taken into account, there seems to be no evidence that lockdown States had better health outcomes: never mind the dramatic picture we should be seeing if lockdown proponents were correct.
As one further example, Japan, although imposing border controls, did not mandate an internal lockdown. The country experienced no excess mortality in 2020, in spite of case numbers increasing. Excess deaths emerged in 2022—after a high proportion of the population was vaccinated. Prior to this, Japanese people simply didn’t die of COVID in high enough numbers to impact excess mortality. This is hard for not only lockdown advocates to explain—but for proponents of the viral theory in general.
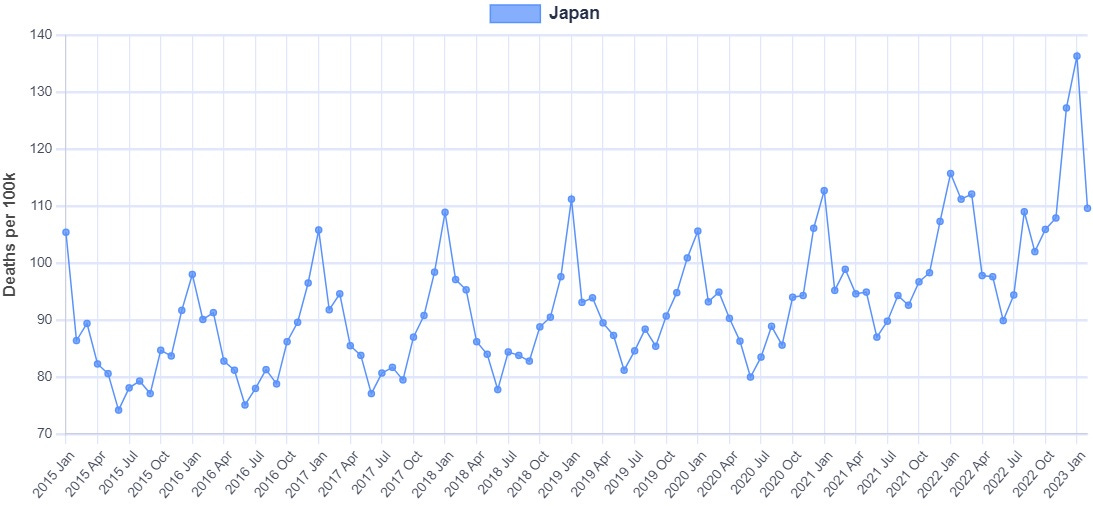
Japan did have a high level of compliance with the Government requests to minimise social contact. This might be expected, if people believe a deadly virus is being breathed out by their fellow humans, then they are likely to avoid them.
Conclusion
In an article explaining the difficulties of assessing lockdown efficacy, Associate Professor of Medicine Vinay Prasad wrote that:
‘I suspect that for many restrictions -- perhaps even most restrictions -- we will never know. We will never know, for instance, if removing the rim from a basketball hoop or closing a toboggan hill slowed SARS-CoV-2 where these strategies were deployed. For larger interventions -- mandatory business closure and stay at home orders, colloquially called "lockdowns" -- we may someday have a scientific consensus as to whether and to what degree this practice changes viral spread, but I believe that day is years away.’
Dr. Prasad writes a perceptive and thought provoking article describing the difficulties of this kind of analysis. If he is correct that lockdowns effects, even on viral spread, are too small to be measured, then this is not a neutral conclusion, rather, it is utterly damning.
If lockdowns came at no cost, then it wouldn’t really matter if the benefit was too small to measure. We know however, that the cost was staggering. Anything less than at least equally staggering benefits then, is an unparalleled disaster. It is clear that lockdowns simply have not demonstrated anything like the kind of benefit that would justify their cost, it is not actually clear they have demonstrated any benefit at all.
Unlike the lockdown predictions, predictions of disaster clearly turned out to be true, with the UN and Oxfam reporting the impact on global poverty and food prices. Cancer diagnoses were missed, elderly people died alone. There are other costs too: unfortunately we do not live in a Disney movie where true love always finds a way. Missed opportunities cannot necessarily be replaced. The obstruction of lockdowns means families that would have otherwise formed, now will not. This is quite an incredible thing to take away from people.
We also do not live in a world where resources can be brought forth by magic. Resources consumed today are simply not there for tomorrow. Lockdowns are a double-whammy, where resources are consumed to pay for people to not create more resources. Countries spent simply vast amounts of money furloughing workers who—as Sweden shows—were at no risk from COVID relative to other health risks they may face. Even if it were possible to keep a country ‘COVID free’ with such a policy, it will simply be paid for in the future when those resources, already spent, are not there to invest in healthcare targeting cancer and heart disease etc. This not to mention any other area of life. There is no world in which it makes sense to redirect resources away from more serious and toward less serious threats to health. This is exactly what governments around the world have done. The United Kingdom now has a consistently higher excess mortality rate than pre-COVID, and this is attributed to strain on the NHS. People are now dying as the resources that would have treated them have already been consumed protecting them from something that posed no comparative threat.
This chapter can only conclude with Tacitus’ famous observation of the Roman Empire, that ‘where they make a desert, they call it peace.’
Read the following chapter, on vaccines, here.
This article is the first chapter of Measuring the Mandates: Questioning the State’s Response to COVID-19. The full book is available here.