


Measuring the Mandates: Viral Origins
Measuring the Mandates: Viral Origins

This article is the first chapter of Measuring the Mandates: Questioning the State’s Response to COVID-19. The full book is available here.
‘99 red balloons Floating in the summer sky Panic bells, it's red alert There's something here from somewhere else The war machine springs to life Opens up one eager eye Focusing it on the sky The 99 red balloons go by’ Nena
In this document so far we have examined the various policies that were mandated to stop the spread of COVID-19. We have questioned whether these mandates were effective, or whether they actually brought about the deaths they ostensibly sought to curb.
At some point it behoves us to ask, what is all of this based upon? What safety signal emerged from China at the turn of the decade that convinced the world a deadly virus was circulating?
Whilst there are reports of Chinese citizens becoming infected with COVID-19 in November of 2019, ‘patient zero’ is considered to have developed symptoms on the 1st of December. The first hospitalisation, retroactively confirmed to be a COVID-19 case, happened around a week after that.
By the 31st of December, tests had been run to identify if a novel infectious agent was behind these cases. The Wuhan Municipal Health Commission released a briefing about early signs of a pneumonia outbreak in the city, which was picked up by various Chinese news agencies.
In response to this, both Hong Kong and Taiwan tightened their inbound screening processes. This is also when the US CDC claims to have first learned of a ‘cluster of 27 cases of pneumonia’ in Wuhan. The following day, US CDC Director Robert Redfield was reportedly ‘rattled’, after being briefed about the severity of the virus. The United Nations then activated its ‘incident-management system’ and China reported the virus to the World Health Organization. The US CDC offered to send experts to assist the investigation. On the 3rd of January, the BBC reported on the ‘mysterious viral pneumonia which has infected dozens of people in the central city of Wuhan’.
It was on this day that Chinese scientists claimed to have ruled out the possibility of various common respiratory pathogens, and identified the genetic sequence of three distinct strains of a novel coronavirus. This was confirmed as the cause of the viral pneumonia cluster on January 6th. The New York Times now reported on the outbreak. Chinese President Xi Jinping ‘made requests for the prevention and control work of the coronavirus outbreak’ at the Politburo of the Chinese Communist Party.
All of this occurred without a single death being attributed to COVID-19.
This raises many questions—questions that were perhaps lost after the dramatic spikes in death rates around the world drew attention. Depending on where you draw the boundary, Wuhan is a city of approximately nine million people, comparable in population to New York. During the especially bad season of 2018, over 23 thousand New Yorkers were hospitalised with flu. At its peak there were over 18 thousand laboratory confirmed cases in one week. It’s reasonable to assume the death toll from this would have substantially contributed to the several thousand deaths the city sees during an average winter month.
At the point President Xi was taking steps to control the outbreak, the WHO and CDC were getting prepared, and the BBC and New York Times started reporting on it, there were a grand total of zero fatalities and 59 cases.
At the risk of labouring the point, the graph below shows the excess mortality in Germany in March of 2018.

Somehow, Germany suffered an astounding 17,087 excess deaths in one single month. Yet, to the best of our knowledge, there is no sign that this caused international alarm. Markets were not closed down and disinfected, the CDC did not intervene, the international media did not run with the story. If a signal this strong does not draw the world’s attention, why was everyone so concerned about a disease that had zero deaths in China?
News reports from the time do not explain this. Initially, it might have been assumed that the Chinese were picking up on highly unusual symptoms. This may have seemed plausible, as not long after, stories appeared in the international media which implanted the idea of a highly unusual virus in the popular imagination.
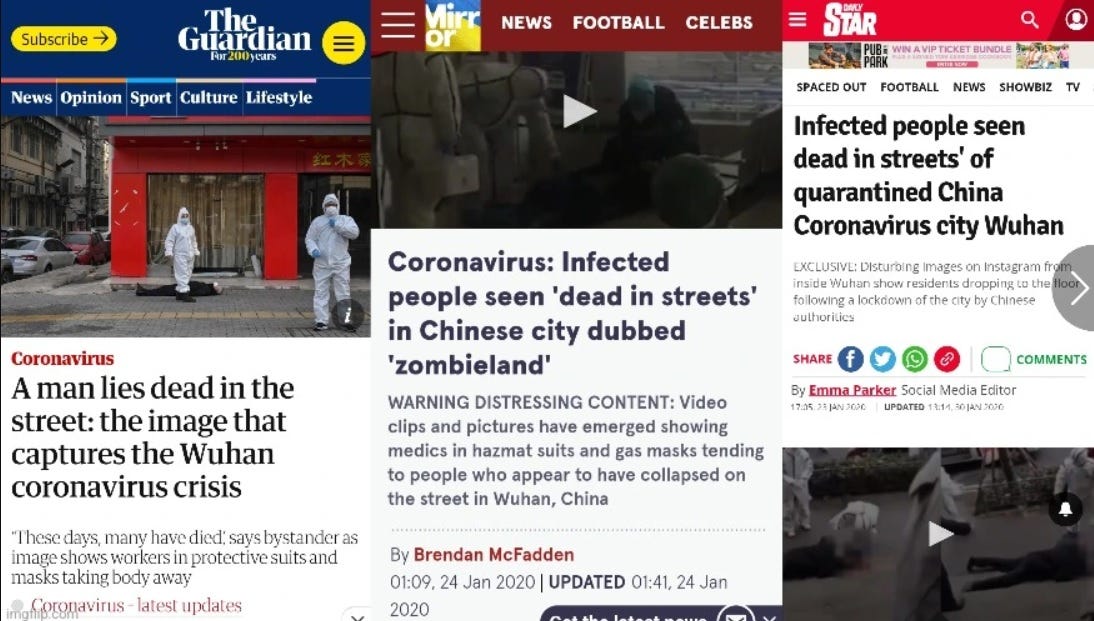
It soon became apparent however, that videos of people walking along the street then suddenly collapsing, were fake. In reality, and as the CDC confirms, COVID cannot be differentiated from the flu by symptoms alone:
‘You cannot tell the difference between flu and COVID-19 by the symptoms alone because they have some of the same signs and symptoms. Specific testing is needed to tell what the illness is and to confirm a diagnosis.’
The question remains then, what did Chinese doctors observe that indicated the presence of a novel virus?
On the 3rd of January, Chinese scientists determined the genetic sequence of the virus they called COVID-19. Within two weeks, the WHO had published a test protocol capable of identifying this new virus.
Everything that follows rests on these two pillars: that a novel virus was accurately identified, and that a polymerase chain reaction (PCR) test could accurately identify it. It was in the belief in the solidity of these pillars that countries around the world enacted mass testing and went into lockdowns. Both of these pillars involve complex science that the vast majority of people—including the media reporting on COVID and the politicians legislating for it—simply do not understand. At best, they have a very limited understanding, one that is reliant on chosen experts who they are unable to critique. If either of these pillars are flawed, the entire COVID narrative comes crashing down.
It is perhaps worth pausing for a moment to reflect that countries around the world took the most drastic cause of action, with the most incredibly far reaching consequences, based on science so few of us understand, and must essentially take on faith alone.
Amongst those who do understand it, this science is not without its critics. A team of twenty two scientists, led by molecular biologist Peter Borger, submitted a retraction request to the journal that published the original PCR protocol. They cited ‘numerous technical and scientific errors’, the most major of which was that the test was based on theoretical sequences of the virus, supplied by a laboratory in China, as none of the actual virus was available.
Borger’s team also highlights the problem of cycle thresholds. PCR tests amplify genetic material, and if the level of amplification is to high, the result becomes meaningless:
‘In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture [reviewed in 2]; if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97%.’
This is in line with comments made by the inventor of PCR, Dr. Kary Mullis, who said:
‘With PCR, if you do it well, you can find almost anything in anybody. It starts making you believe in the sort of Buddhist notion that everything is contained in everything else. If you can amplify one single molecule up to something which you can really measure, which PCR can do, then there’s just very few molecules that you don’t have at least one single one of them in your body, okay. So that could be thought of as a misuse of it, just to claim that it’s meaningful… PCR is just a process that’s used to make a whole lot of something out of something. That’s what it is. It doesn’t tell you that you’re sick and it doesn’t tell you that the thing you ended up with really was going to hurt you or anything like that.’
As a substantial critique of the scientific underpinning of the PCR test is beyond the scope of this paper, more extensive resources are therefore provided in the endnotes.
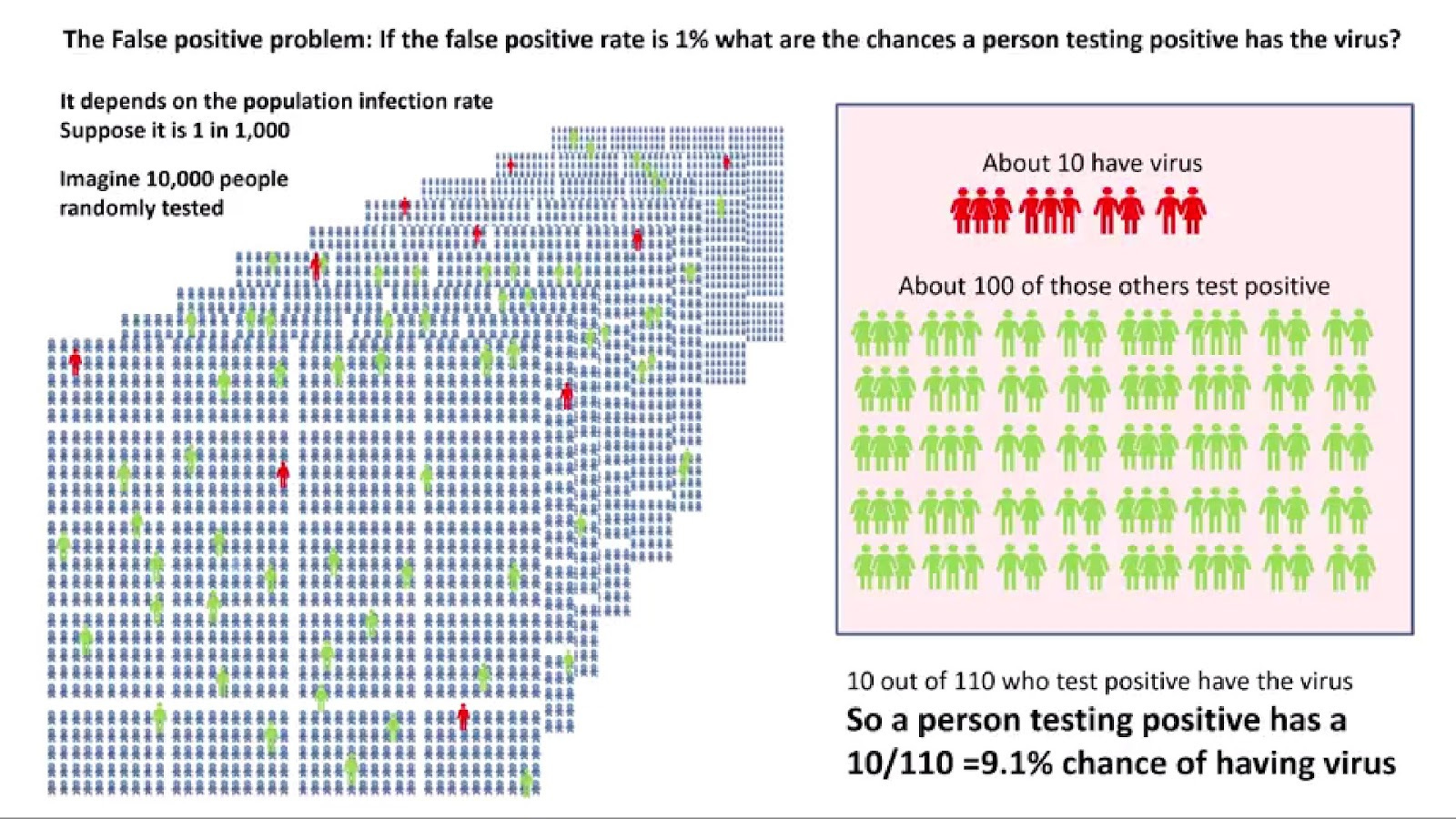
In addition to the scientific issues, there is also a purely mathematical problem with the accuracy of tests. If a test has a mere 1% false positive rate, it would seem like a person testing positive has a 99% chance of having the virus. Perhaps counter-intuitively, this is not the case, in fact the actual probability cannot be known without first knowing the prevalence of the virus in society.
As a thought experiment: imagine a society of 10 thousand people, where only 10 have contracted a certain virus. If everyone in this society took a 99% accurate test, the 10 infected would get positive results, but due to the 1% false positive rate, so would 100 uninfected people, making a total of 110. A person testing positive therefore has a 9.1% chance of actually being positive, not 99%. This obviously has damning implications for the use of PCR, given that the tests were used to stop people from leaving their homes etc.
An example of what can go wrong with PCR occurred in 2006, in what The New York Times later described as the ‘epidemic that wasn’t’. This incident took place at the Dartmouth-Hitchcock Medical Center, in New Hampshire. It began when several healthcare workers developed a cough, and an infectious disease expert became concerned this signalled the beginning of a whooping cough epidemic. This was a concerning issue, as whooping cough would represent a serious threat to the hospital vulnerable patients. The New York Times reported that:
‘For months, nearly everyone involved thought the medical center had had a huge whooping cough outbreak, with extensive ramifications. Nearly 1,000 health care workers at the hospital in Lebanon, N.H., were given a preliminary test and furloughed from work until their results were in; 142 people, including Dr. Herndon, were told they appeared to have the disease; and thousands were given antibiotics and a vaccine for protection. Hospital beds were taken out of commission, including some in intensive care.
‘Then, about eight months later, health care workers were dumbfounded to receive an e-mail message from the hospital administration informing them that the whole thing was a false alarm.’
Laboratory tests failed to confirm a single case of whooping cough. It appears the healthcare workers simply had ordinary respiratory diseases, such as the common cold. The outbreak of this pseudo-pandemic was attributed to placing too much faith in highly sensitive molecular tests. It is reasonable to assume that the furlonging of healthcare workers and reduction of hospital beds would have had real consequences on health outcomes.
Throughout the ages, human literature has warned of the perils of self-fulfilling prophecies. From the ancient Greek myth of Oedipus, through Shakespeare's Macbeth, to the modern myths of Harry Potter and Star Wars. Perhaps there is a reason for this beyond simply making a compelling story. The quotation from the start of this chapter is a verse from the song 99 Red Balloons. It tells the story of a nation mistaking these balloons for an enemy invasion, and readying its war machine. Seeing this, the suspected invader concludes it is under threat, and readies its own machine. The first nation takes this as confirmation that it was right all along, and war ensues.
The song reflects the sense of meaning the conflict brings. Lines like ‘This is what we've waited for, This is it boys, this is war’, illustrate how entire bureaucracies now find justification for their existence, whilst ‘Everyone's a superhero, Everyone's a Captain Kirk,’ speaks to how people are lifted out of the mundanity of life into a heroic narrative. It all ends in disaster however, as the singer is left ‘In this dust that was a city’, looking for a souvenir, ‘Just to prove the world was here’.
Has COVID-19 been such a ‘red balloon’? Has what happened at the Dartmouth-Hitchcock Medical Center simply played out on a global scale? Did we get into a vicious circle, where PCR tests were used to justify lockdowns, which caused a surge in excess deaths, which was taken as evidence that the tests were indeed right?
To repeat the conclusion of Chapter One: it is not within the scope of this document to draw grand conclusions to such questions. It is well within all of our scopes however, to assert that this remains the most centrally important question that we must all seek to answer.
Read the Conclusion, here.
This article is the first chapter of Measuring the Mandates: Questioning the State’s Response to COVID-19. The full book is available here.